Japan implemented its nationwide vaccination program against COVID-19 in 2021, immunizing more than one million people (approximately 1%) a day. However, the direct and indirect impacts of the program at the population level have yet to be fully evaluated. To assess the vaccine effectiveness during the Delta variant (B.1.617.2) epidemic in 2021, we used a renewal process model. A transmission model was fitted to the confirmed cases from 17 February to 30 November 2021. In the absence of vaccination, the cumulative numbers of infections and deaths during the study period were estimated to be 63.3 million (95% confidence interval [CI] 63.2–63.6) and 364,000 (95% CI 363–366), respectively; the actual numbers of infections and deaths were 4.7 million and 10,000, respectively. Were the vaccination implemented 14 days earlier, there could have been 54% and 48% fewer cases and deaths, respectively, than the actual numbers. We demonstrated the very high effectiveness of COVID-19 vaccination in Japan during 2021, which reduced mortality by more than 97% compared with the counterfactual scenario. The timing of expanding vaccination and vaccine recipients could be key to mitigating the disease burden of COVID-19. Rapid and proper decision making based on firm epidemiological input is vital.

Vaccination against coronavirus disease (COVID-19) was widely implemented at nationwide and global scale; therefore, its evaluation at population level, including direct and indirect effects, is key for assessing this policy program 1,2,3 . For instance, Japan implemented a nationwide vaccination program against COVID-19 in 2021 using mRNA vaccines and prioritizing health care professionals from February 2021, then older adults aged ≥ 65 years and those with underlying comorbidities, followed by younger individuals. For mass vaccination, the Pfizer/BioNTech mRNA vaccine (BNT162b2) using ancestral severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) strain was utilized. The Moderna vaccine (mRNA-1273) was also used for a part of the vaccination rollout and also for vaccination in the workplace. Immunization was conducted to cover more than one million people (approximately 1%) a day when the pace of vaccination was at its peak. Therefore, post-hoc evaluation is essential to understand how influential the program was at population level. Alongside the vaccination program, various public health and social measures (PHSM) were implemented, including the declaration of the state of emergency and contact tracing 4 . These measures aimed to suppress virus transmission even temporarily, thereby alleviating the burden on healthcare facilities and protecting the health infrastructure. Despite these efforts, the virus posed significant challenges, partly due to the emergence of new variants with elevated transmissibility including Alpha (B.1.1.7) and Delta (B.1.617.2) variants, imposing additional difficulties in controlling the spread of SARS-CoV-2 5,6,7 .
In evaluating the indirect effects of vaccination owing to reduced opportunities for infection and decreased transmissibility (e.g., herd immunity effect), the epidemiological evaluation of population-level effectiveness calls for statistical methods 8,9,10,11 . For direct effects only (i.e., whether vaccinated individuals are protected biologically by comparing vaccinated and unvaccinated people), the estimation is simpler, as reported in many countries 12,13,14,15,16 , including estimates in Japan 17 . However, evaluation of population-level effects are scarce (mainly in the United States and Israel) 18,19 , although global estimates have been reported 20 . Whereas the indirect effectiveness of vaccination has been understudied, the related published studies imply that the impact of herd immunity has been substantial during the pre-Omicron period of the COVID-19 pandemic 18,19 .
The present study is focused on the post-hoc evaluation of the vaccination program in Japan where the mortality impact of COVID-19 has been one of the lowest among countries belonging to the Organization for Economic Cooperation and Development 21 . Calculating the counterfactual scenario, herein, we aimed to estimate the total effectiveness of COVID-19 vaccination in Japan in 2021, during which the course of the primary series of the vaccination program was completed and third dose (or booster dose) was not administered yet. We further examined scenarios involving different timing and recipients of vaccination.
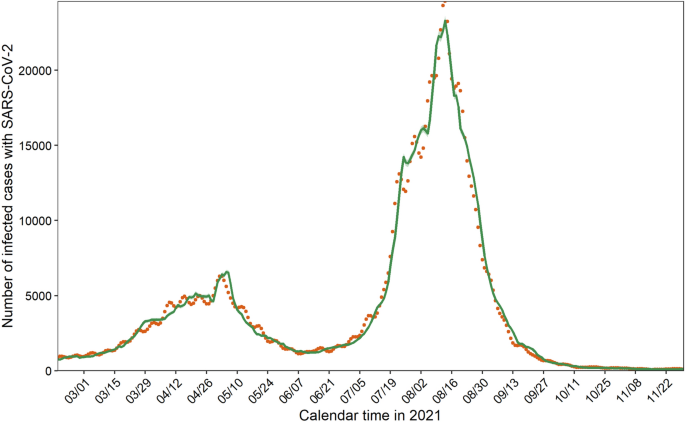
Addressing age-dependent heterogeneity along with vaccination coverage, our transmission model successfully captured the observed data during the primary series of the vaccination program in Japan (Fig. 1 and Supplementary Fig. S8). Whereas the prototype model in Fig. 1 unrealistically assumed that observed cases represented all infected individuals (i.e., ascertainment bias factor at 1), hereinafter, we present results using other plausible reporting coverages, i.e., 0.125, 0.25, and 0.50, as shown in Supplementary Fig. S9 and Supplementary Table S1.
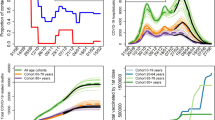
Hypothetical cumulative numbers of infections and deaths from February to November 2021 were explored in the absence of vaccination by different reporting coverages (Table 1). We found that the cumulative number of infections differed, from 63.3 million (95% CI 63.2–63.6) to 72.0 million (95% CI 71.4–72.6) cases for reporting coverages of 0.25 and 0.50, respectively. The possible cumulative number of deaths without vaccination ranged from 213,000 (95% CI 212–213) to 860,000 (95% CI 850–869) deaths for reporting coverage from 0.125 to 0.50. Compared with variations in cases, variations in deaths were broader because the infection fatality risk also varied by reporting coverage (Supplementary Figs. S10 and S11).
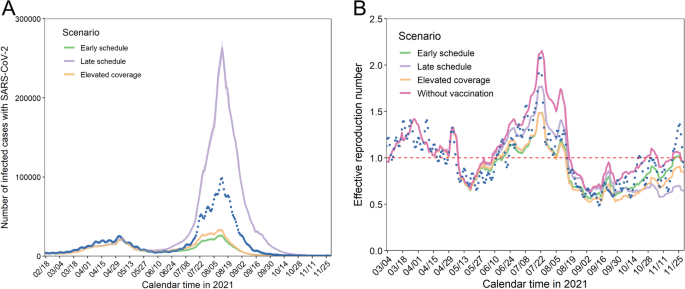
Table 2 presents the cumulative number of infections with SARS-CoV-2 by age group and counterfactual scenario. Whereas the early schedule and elevated coverage scenarios respectively could have contributed to reductions of 54% and 47% overall, the late schedule scenario could have led to an increase in infections of 117%, reaching more than 10 million infections by the end of November 2021. In all examined scenarios, young adults aged 20–29 years yielded the greatest number of infections whereas the relative and absolute reductions with better vaccination programs than the actual program were comparable among people aged 10–49 years.
Table 2 Cumulative numbers of infections with SARS-CoV-2 in the counterfactual scenarios.The cumulative numbers of deaths by age group and counterfactual scenario are summarized in Table 3. Mortality in older people was more sensitive to different vaccination scenarios. In the late schedule scenario, the relative increase in the number of deaths was estimated to be 50%, i.e., this scenario yielded more than 5000 additional deaths by the end of November 2021.
Table 3 Cumulative numbers of deaths associated with COVID-19 in the counterfactual scenarios.Whereas Japan successfully implemented its primary series of vaccination against COVID-19, reaching 75% coverage by the end of November 2021 23 , a pressing question has been how successful the program was during the pre-Omicron period. The present study revealed that without the vaccination program, the cumulative numbers of infections and deaths would have been 63.3 million (95% CI 63.2–63.6) and 364,000 (95% CI 363–366), respectively, assuming that confirmed cases represented 25% of infections. Despite the immense impact of the program, had vaccination been implemented 14 days earlier, there could have been 54% and 48% fewer cases and deaths, respectively, than the observed numbers. These figures represent the averted number of cases and deaths, and such estimates contrast to vaccine effectiveness (or efficacy) estimate at an individual level via randomized controlled trial or cohort study design, i.e., the averted number estimates require the vaccination coverage at the population level (possibly in real time), and additional datasets, including transmission dynamics, need to be analyzed to clarify the indirect effect of vaccination. The use of renewal process models enabled us to demonstrate the critical importance of the pace of the vaccination program and the prioritizing of vaccine recipients in determining the disease burden associated with COVID-19.
A critical take-home message from the present study is that the indirect effect of vaccination was enormous in Japan. The numbers of prevented infections and deaths were 13.5 and 36.4 times the empirically observed counts, respectively. In other words, the total effectiveness of the vaccination program in preventing infection and death was estimated at 92.6% and 97.2%, respectively. Of these fractions, the direct effect (i.e., comparison of risks between vaccinated and unvaccinated cases) that we estimated earlier 17 accounted for only 3.6% and 5.1%, respectively, and the indirect effect (i.e., comparison of risks between actual and counterfactual courses of the epidemic) was as large as 89.0% and 92.1% reductions in infections and deaths, respectively. Such differences were seen because the incidence in Japan remained relatively lower than those in Western countries owing to PHSM, e.g., less than 5% of the population was reported as a COVID-19 case by the end of 2021. Clarifying the total effectiveness of vaccination was facilitated by modeling to yield the counterfactual scenario, and our finding regarding the total effect echoes those of published studies 18,19 . Together with past evidence 18,19 , consistent findings that the vaccination program prevented infections among half of the Japanese population and more than 90% of prevented deaths were owing to its indirect effect indicate that the vaccination program was enormously successful during the Delta variant epidemic wave during 2021 in Japan. The importance of indirect effect is what the present study contrasts to existing published studies 12,13,14,15,16,17 that only directly measured individual benefit of vaccination, including the averted cases, hospitalization, severe complication and death. In many countries with greater incidence, including Brazil 15 , Israel 14 , Italy 12 , United States 16 and countries that belong to WHO European Region 13 , the direct effect was already enormous. Japan enjoyed smaller incidence by the end of 2021 and the direct effect was relatively limited 17 , but the present study has been unique in that it demonstrated that the indirect effect can be inferred to be substantial using the effective reproduction number in a counterfactual scenario.
Another notable finding of this study is that our modeling approach enabled us to examine hypothetical scenarios in which the vaccination pace is accelerated. The cumulative numbers of infections in the early schedule and late schedule scenarios were estimated to be 2.2 million (95% CI 2.0–2.3) and 10.2 million (95% CI 9.8–10.6), respectively, which clearly led to substantial differences in mortality. Epidemiological studies can help policy makers recognize that a 1- or 2-week difference in the implementation of vaccination could yield completely different population impacts.
Published studies have indicated that prioritized vaccination for older people could minimize COVID-19 mortality if vaccines are not sufficiently available 24,25,26,27,28 . This was consistent with our finding, i.e., the early schedule scenario yielded better outcomes than the elevated coverage scenario. However, in our elevated coverage scenario (i.e., encouraging more adolescents and people aged 10–59 years to be vaccinated), the total effect was substantial, even when older people were not prioritized for vaccination. This demonstrates that vaccinating younger individuals with substantial transmission potential is a critical strategy in mitigating the magnitude of the epidemic for an entire population, including children aged < 10 years who were not eligible for the vaccination program. Taken together, the present study findings imply that, given a substantial vaccine supply and immunization capacity, allocating vaccines for younger adults in addition to prioritizing older adults could reduce the overall COVID-19 burden, as previously indicated 19,27,29,30,31,32 .
So, how should we rate the vaccination program in Japan during the SARS-CoV-2 Delta variant epidemic wave? The Japanese government set a goal for the daily number of vaccinated people of one million in early May 2021 (which was achieved from late June to July), subsequently stating that the maximum number was to be 1.5 million in the later part of the same month 33 . In addition to mass vaccination with initial prioritization of older people and health care workers, the program of vaccination in the workplace aimed at expanding coverage started in late June 2021 34 . Our counterfactual scenario indicated that the observed vaccination program helped avoid the worst case. However, if the vaccination program had begun 2 weeks later than the observed schedule, substantial mortality could have occurred. Additionally, a surge in COVID-19 patients observed in July–September 2021 was the largest epidemic wave ever experienced in Japan, and the corresponding period fell under the state of emergency, which was based on a non-legally binding policy in which the government requested voluntary restriction of contacts 35 . Were PHSM not in place under the state of emergency, the number of infections could have been even greater than the observed number. Considering that our early schedule and elevated coverage schedule scenarios were realistic in their anticipated pace of vaccination, considerable mortality and resulting economic losses could have been mitigated. Perhaps more importantly, from a scientific point of view, evidence regarding the indirect impact of such interventions in real time using modeling techniques should be routinely accessible to policy makers during future pandemics.
Our study involved several technical limitations. First, as previously mentioned, during the research period, Japan experienced three state of emergency declarations: from 8 January to 21 March, from 25 April to 20 June, and from 12 July to 30 September 2021. Rather than incorporating the specific variable of a state of emergency into the model (e.g., quantified effectiveness of PHSM), we tried to indirectly capture its impact via estimating the effective reproduction number using several explanatory variables, including mobility. In fact, use of human mobility data as a predictor is recognized as reflecting the impact of PHSM 36,37,38,39 . It should be noted, however, that published studies have attempted to measure the population-level impact of both vaccination and PHSM over the course of time 40,41 . Second, the contact matrix used in the present study was quantified before the study period 42 , and the next-generation matrix was calibrated during the course of the pandemic. At minimum, our time-dependent reproduction number helped capture the transmission dynamics over time and across ages (Fig. 1). Third, vaccine-induced immunity and immunity following natural infection were dealt with independently in the present study, and we did not account for the effect of waning immunity with the latter during the study period. We focused on the period shortly after vaccination and before the vaccination rollout, when approximately only 1% of the population experienced COVID-19 infection. Fourth, we did not take into account the heterogeneities over geographical space. Strictly speaking, the state of emergency covered different durations and areas according to prefecture, leading to specific variations in mobility information 43 . Finally, while vaccines against the Omicron variant, which is antigenically distinct, have shown reduced effectiveness compared to previously circulating variants 44,45 , the population-level impact of those changes have yet to be understood well 46 . In line with this, we have yet to understand whether the indirect effects of vaccination continued to accumulate and played a pivotal role in responding to the Omicron variant and its subvariants, including XBB. Future studies should address the issue of population impact during Omicron era.
We demonstrated that the indirect effect of vaccination in Japan during 2021 was very large, with the vaccination program reducing mortality by more than 97%. The pace of vaccination and prioritization of vaccine recipients have been key to mitigating the mortality burden of COVID-19. In the future, firm and prompt policy-making process based on real-time understanding of the transmission dynamics under various vaccination scenarios is called for.
COVID-19 was designated a notifiable disease under the infectious disease law of Japan as of 2021. All individuals suspected of being infected with SARS-CoV-2 were tested via PCR or quantitative antigen test at medical facilities. They were then requested to remain in home isolation and undergo investigation by municipal public health centers to identify their close contacts. Information of confirmed cases (e.g., age and sex) was registered in the Health Center Real-time Information-sharing System on COVID-19 (HER-SYS) by medical facilities or municipal public health centers. Supplementary Fig. S1A shows the number of confirmed cases from the beginning of the primary series (the first and second doses) of the vaccination program through the end of November 2021. In the end of November 2021, SARS-CoV-2 in Japan was dominated by Delta variant to which the vaccine effectiveness was known to have been greatly diminished, sometimes by 10%, compared with other variants that circulated earlier 47,48,49 .
The time of infection for all confirmed COVID-19 cases retrieved from HER-SYS was backcalculated using a previously estimated distribution of the interval between infection and illness onset, assumed to follow a log-normal distribution with a mean of 4.6 days and standard deviation (SD) of 1.8 days 50, 51 . Cases without a date of symptom onset were backcalculated using the time difference from symptom onset to reporting, assumed to follow a log-normal distribution with a mean of 2.6 days and SD of 2.1 days, as previously estimated using cases with information for the date of symptom onset. Non-parametric backcalculation was performed using the R-package “surveillance” (version 1.20.3). To address the issue of reporting bias, we explored different reporting coverages: 0.125, 0.25, 0.5, and 1.0 (no bias) by multiplying the backcalculated cases by 1 and dividing by reporting coverage to finally obtain the number of infections.
SARS-CoV-2, all vaccinated individuals retrieved from the Vaccine Record System (VRS) were converted into immunized people according to time. The data comprised the sex, age, and date of vaccination for vaccinated individuals. We assumed that all people who received the first dose were subsequently vaccinated with the second dose at an interval of 21 days (Supplementary Fig. S1B). According to statistics of the VRS, there was a very small discrepancy in vaccination coverage between the first dose (75.19%) and the second dose (74.61%) as of the end of December 2021 52 ; therefore, we could obtain a certain consensus on the usage data for people vaccinated with the first dose only. For the conversion, we used a profile of vaccine efficacy involving waning immunity for the primary series used by Gavish et al. 19 , which was based on previous estimates 53,54 . Given the widespread use of the messenger RNA vaccine BNT162b2 (Pfizer/BioNTech) in Japan (more than 80% of individuals received this vaccine by the end of November 2021) 23 , we assumed that published estimates could directly be applied to the case of Japan. Further details and background of the primary series in Japan’s vaccination program are described elsewhere 17 .
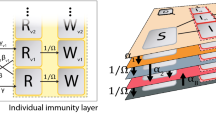
To adapt the following transmission model, we used the number of vaccinated individuals and the profile of vaccine efficacy to estimate the immune fraction in age group \(a\) at calendar time \(t\) , \(_\) , which is expressed as:
$$where \(_\) is the population size in age group \(a\) in 2021 55 , \(_\) denotes the number of vaccinated individuals in age group \(a\) at calendar time \(t\) , and \(_\) represents the vaccine profile. Supplementary Fig. S2 displays the estimated immune fraction by age group.
We developed the time-dependent transmission model that accounts for heterogeneous transmission between age groups, fitting the model to observed incidence data and estimating unknown parameters. We used the following renewal equation to infer the transmission dynamics underlying the COVID-19 epidemic, which is described as: