Although defined in a variety of ways, static exertion generally means the performance of a task from one postural position for an extended duration. The condition is a combination of force, posture, and duration. The degree of risk is in proportion to the combination of the magnitude of the external resistance, awkwardness of the posture, and duration.
A grip is the conformity of the hand to an object accompanied by the application of exertion usually to manipulate the object. Hence, it is the combination of a force with a posture. Grips are applied to tools, parts, and other physical objects in the work setting during task performance. To generate a specific force, a pinch grip requires a much greater muscle exertion than a power grip (object in the palm of the hand). Hence, a pinch grip has a greater likelihood of creating injury. The relationship between the size of the hand and the size of the object also influences risk of injury. Grant et al. (1992) found reduced physical exertion when the handle was one cm less than the subjects’ grip diameter.
Bulky clothes, used to protect the worker from cold or other physical elements, may increase the muscle effort required to perform tasks.
Angular velocity/angular acceleration is the speed of body part motion and the rate of change of speed of body part motion, respectively. Marras and Schoenmarklin (1991, 1993) found a mean wrist flexion/extension acceleration of 490 deg/sec sec in low risk jobs and acceleration of 820 deg/sec sec in high risk jobs. Marras et al. (1995) associated trunk lateral velocity and trunk twisting velocity with medium and high-risk occupationally-related low back disorder.
Repetition is the time quantification of a similar exertion performed during a task. A warehouse worker may lift and place on the floor three boxes per minute; an assembly worker may produce 20 units per hour. Repetitive motion has been associated with injury (Hagberg, 1981; Armstrong et al., 1982) and worker discomfort (Ulin, 1990). Generally, the greater the number of repetitions, the greater the degree of risk. However, the relationship between repetition and degree of injury risk is modified by other risk factors such as force, posture, duration, and recovery time. No specific repetition threshold value (cycles/unit of time, movements/unit of time) is associated with injury.
Recovery time is time quantification of rest, performance of low stress activity, or performance of an activity that allows a strained body area to rest. Short work pauses have reduced perceived discomfort (Hagberg and Sundelin, 1986) and rest periods between exertions have reduced performance decrement (Caldwell, 1970). The recovery time needed to reduce the risk of injury increases as the duration of risk factor increases. Specific minimum recovery times for risk factors have not been established.
The cardiovascular system provides oxygen and metabolites to muscle tissue. Some tasks require long-term/repetitive muscle contraction such as walking great distances, heavy carrying, and repeat lifting. As physical activity increases, muscles demand more oxygen and metabolites. The body responds by increasing the breathing rate and heart rate. When muscle demand for metabolites can not be met (metabolic energy expenditure rate exceeds the body’s energy producing and lactic acid removal rate) physical fatigue occurs. When this happens in a specific area of the body (shoulder muscle from repeat or long term shoulder abduction), it is termed localized fatigue and is characterized by tired/sore muscles. When this happens to the body in general (from long-term heavy carrying/lifting/climbing stairs), it is termed whole body fatigue and may produce a cardiovascular accident. Also, high heat from the environment can cause an increase in heart rate through body cooling mechanisms. Therefore, for a given task, metabolic stress can be influenced by environmental heat.
Vibration applied to the hand can cause a vascular insufficiency of the hands/fingers (Raynaud’s disease or vibration white finger). Also, it can interfere with sensory receptor feedback leading to increased hand grip force to hold the tool. Further, a strong association has been reported between carpal tunnel syndrome and segmental vibration (Silverstein et al., 1987; Wieslander et al., 1989).
Heat stress is the total heat load the body must accommodate. It is generated externally from environment temperature and internally from human metabolism. Excessive heat can cause heat stroke, a condition that can be life threatening or result in irreversible damage. Less serious conditions associated with excessive heat include heat exhaustion, heat cramps, and heat-related disorders (e.g., dehydration, electrolyte imbalance, loss of physical/mental work capacity).
Cold stress is the exposure of the body to cold such that there is a lowering of the body’s deep core temperature. Systemic symptoms that a worker can present when exposed to cold include shivering, clouded consciousness, extremity pain, dilated pupils, and ventricular fibrillation. Cold can also reduce hand grip strength and coordination. As mentioned earlier in the section on Force, bulky clothes and gloves used to protect the worker from cold exposure can increase the muscle effort required to perform tasks.
Exposure of the whole body to vibration (usually through the feet/buttocks when riding in a vehicle) has some support as a risk for injury. Boshuizen et al. (1990) found the prevalence of reported back pain to be approximately 10 percent higher in tractor drivers than in workers not exposed to vibration, and the prevalence of back pain increased with vibration dose. Dupuis (1987) reported that operators of earth-moving machines with at least 10 years of exposure to whole body vibration showed lumbar spine morphological changes earlier and more frequently than non-exposed people.
With industrialization, the trend regarding lighting has been to provide a higher lighting level. This has proven hazardous within certain work settings such as in offices in which problems with glare and eye symptoms have been associated with levels above 1000 lux (Grandjean, 1988). Barreiros and Carnide (1991) found differences in visual functions over the course of a workday among VDT operators and money changers who worked in badly lighted environments. The current recommended trend in office lighting is to have low background lighting (from 300 to 700 lux) coupled with nonglare task lighting which can be controlled with a rheostat. This is consistent with Yearout and Konz’s (1989) findings of operator preference regarding lighting. Work that requires high visual acuity and contrast sensitivity needs high levels of illumination. Fine and delicate work should be illuminated at 1,000 to 10,000 lux (Grandjean, 1988).
Noise is unwanted sound. In the industrial setting, it may be continuous or intermittent and present in various ways (bang of a rifle, clatter of a pneumatic wrench, whirl of an electric motor). Exposure to noise can lead to temporary and permanent deafness, tinnitus, paracusis, or speech misperception. The louder the noise and the greater its duration, the greater the risk to hearing. Also, noise well below thresholds that cause hearing loss may interfere with the ability of some people to concentrate.
Several approaches are used to identify the existence of ergonomic risks. The method used depends on the managerial philosophy of the company (getting workers involved through a participatory process versus top/down process), level of analysis (one job versus company wide evaluation), and personal preference. There is no one correct approach.
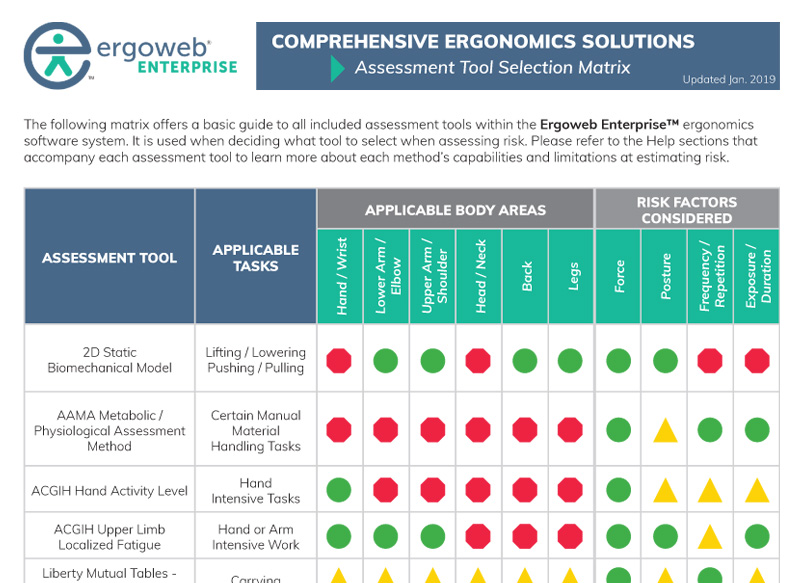
Once the presence of risk factors is established, the degree of risk associated with those factors is evaluated. This is done through the application of analytical ergonomic tools and the utilization of specific guidelines. Ergonomic Assessment and Analysis Tools There are a variety of analytical tools, and they are usually orientated to a specific type of task or job (e.g., manual material handling) or a particular body part (e.g., wrist, low back). Analytical tools also vary greatly in their style of conclusions. They may provide job prioritization for intervention, quantification of activities associated with increased risk of injury, or recommendation for a load weight limit for lifting. The examiner determines which analytical tool is best for evaluation of the identified risks based on an understanding of the tool’s applications, strengths, and weaknesses. An analytical tool can provide an estimate of injury risk. Variation in individual physiology, history of injury, work methods, and numerous other factors influence whether a person will sustain an injury. You can download a comprehensive list of assessment and analysis tools — here’s a snapshot:
Many more ergonomics tools are listed in the literature. Hagber et al. (1995) and Louhevaara (1995) provide information on several of them.
Engineering controls involve altering the physical items in the workplace, including actions such as modifying the workstation, obtaining different equipment, or changing tools. The focus of engineering controls involves identifying the underlying stressor (risk factor of awkward posture, force, repetition, etc.) and eliminating it through changing the physical environment. For example, a video display terminal worker who sustains a shoulder/neck complaint from long-term typing may need forearm supports or a keyboard tray to reduce the long-term, static exertion of neck/shoulder muscles. Engineering controls are the preferred method of risk control because they permanently reduce or eliminate the risk.
Work practice controls involve training and encouraging a specific method of task performance to reduce worker exposure to the ergonomic risk. An example of work practice control is training workers in proper lifting techniques.
In the US, several standards and guidelines are available. OSHA Ergonomics Program Standard Standards (e.g., ISO 6385: Ergonomic principles in the design of work systems) and Guidelines (e.g., ANSI B11 TR 1-1993: Ergonomic Guidelines for the Design, Installation and Use of Machine Tools, ANSI Z-365: Control of Work-Related Cumulative Trauma Disorders) note a risk of injury is associated with postural position. This article was updated on May 15, 2019.